What Is Bursitis In The Foot?
Overview
Pain at the posterior heel or posterior ankle is most commonly caused by pathology at the posterior calcaneus, the Achilles (calcaneal) tendon, or the associated bursae. The following bursae are located just superior to the insertion of the Achilles tendon. Subtendinous calcaneal bursa. This bursa (also called the retrocalcaneal bursa), situated anterior (deep) to the Achilles tendon, is located between the Achilles tendon and the calcaneus. Subcutaneous calcaneal bursa. Also called the Achilles bursa, it is found posterior (superficial) to the Achilles tendon, lying between the skin and the posterior aspect of the distal Achilles tendon. Inflammation of one or both of these bursae can cause pain in the posterior heel and ankle regions.
Causes
Overuse of the ankle joint may cause irritation of the bursa such as excessive walking, running or jumping. Poor biomechanics and foot function may ultimately lead to heel bursitis due to pulling on the back of the heel by the Achilles tendon.
A sudden increase in physical activity without adequate rest may result in heel bursitis. Excessive standing and walking bare foot on hard surfaces.
Symptoms
Pain when activating the Achilles tendon (running and jumping) and when applying pressure at the point of attachment of the tendon on the heel bone. Contrary to the tenderness occurring with inflammation of the Achilles tendon, the tenderness is localised to the point of attachment to the heel bone.
Diagnosis
Like all other forms of bursitis, initially the physician will take down the history of symptoms experienced by the patient, this will be followed by a detailed physical examination which involves checking for inflammation signs like pain, redness, and warmth of the heel area. The physician might examine further by moving the ankle a little to determine the exact location of pain. Further diagnostic tests including x-ray, bone scans, and MRI scan might be suggested if required.
Non Surgical Treatment
Medications may be used to reduce the inflammation and pain of retrocalcaneal bursitis. Nonsteroidal anti-inflammatory drugs such as ibuprofen, naproxen and ketoprofen can be purchased without a prescription and used to treat mild to moderate pain. These drugs are often used in combination with a physical therapy program or other retrocalcaneal bursitis treatments.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Pain at the posterior heel or posterior ankle is most commonly caused by pathology at the posterior calcaneus, the Achilles (calcaneal) tendon, or the associated bursae. The following bursae are located just superior to the insertion of the Achilles tendon. Subtendinous calcaneal bursa. This bursa (also called the retrocalcaneal bursa), situated anterior (deep) to the Achilles tendon, is located between the Achilles tendon and the calcaneus. Subcutaneous calcaneal bursa. Also called the Achilles bursa, it is found posterior (superficial) to the Achilles tendon, lying between the skin and the posterior aspect of the distal Achilles tendon. Inflammation of one or both of these bursae can cause pain in the posterior heel and ankle regions.
Causes
Overuse of the ankle joint may cause irritation of the bursa such as excessive walking, running or jumping. Poor biomechanics and foot function may ultimately lead to heel bursitis due to pulling on the back of the heel by the Achilles tendon.
A sudden increase in physical activity without adequate rest may result in heel bursitis. Excessive standing and walking bare foot on hard surfaces.
Symptoms
Pain when activating the Achilles tendon (running and jumping) and when applying pressure at the point of attachment of the tendon on the heel bone. Contrary to the tenderness occurring with inflammation of the Achilles tendon, the tenderness is localised to the point of attachment to the heel bone.
Diagnosis
Like all other forms of bursitis, initially the physician will take down the history of symptoms experienced by the patient, this will be followed by a detailed physical examination which involves checking for inflammation signs like pain, redness, and warmth of the heel area. The physician might examine further by moving the ankle a little to determine the exact location of pain. Further diagnostic tests including x-ray, bone scans, and MRI scan might be suggested if required.
Non Surgical Treatment
Medications may be used to reduce the inflammation and pain of retrocalcaneal bursitis. Nonsteroidal anti-inflammatory drugs such as ibuprofen, naproxen and ketoprofen can be purchased without a prescription and used to treat mild to moderate pain. These drugs are often used in combination with a physical therapy program or other retrocalcaneal bursitis treatments.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Do Hammer Toes Cause Numbness
 Overview
Overview
hammertoe can occur when feet are crammed into shoes so tight that the front of the toes are pushed against the front of the shoes for prolonged periods of time. One or more toes then remain bent with the middle knuckle pointing up, even when shoes are taken off. If the condition is left untreated and tight footwear is continually worn, these bent toes can become so rigid that they can no longer straighten out on their own. While any shoes that are too tight can lead to this condition, high heels seem to be a big culprit since the elevated ankle causes more weight to push the toes forward. This may explain why the condition affects more women than men.
Causes
If a foot is flat (pes planus, pronated), the flexor muscles on the bottom of the foot can overpower the others because a flatfoot is longer than a foot with a normal arch. When the foot flattens and lengthens, greater than normal tension is exerted on the flexor muscles in the toes. The toes are not strong enough to resist this tension and they may be overpowered, resulting in a contracture of the toe, or a bending down of the toe at the first toe joint (the proximal interphalangeal joint) which results in a hammertoe. If a foot has a high arch (pes cavus, supinated), the extensor muscles on the top of the foot can overpower the muscles on the bottom of the foot because the high arch weakens the flexor muscles. This allows the extensor muscles to exert greater than normal tension on the toes. The toes are not strong enough to resist this tension and they may be overpowered, resulting in a contracture of the hammertoes toe, or a bending down of the toe at the first toe joint (the proximal interphalangeal joint) which results in a hammertoe.
 Symptoms
Symptoms
If the toes remain in the hammertoe position for long periods, the tendons on the top of the foot will tighten over time because they are not stretched to their full length. Eventually, the tendons shorten enough that the toe stays bent, even when shoes are not being worn. The symptoms of hammertoe include a curling toe, pain or discomfort in the toes and ball of the foot or the front of the leg, especially when toes are stretched downward, thickening of the skin above or below the affected toe with the formation of corns or calluses, difficulty finding shoes that fit well. In its early stages, hammertoe is not obvious. Frequently, hammertoe does not cause any symptoms except for the claw-like toe shape.
Diagnosis
The exam may reveal a toe in which the near bone of the toe (proximal phalanx) is angled upward and the middle bone of the toe points in the opposite direction (plantar flexed). Toes may appear crooked or rotated. The involved joint may be painful when moved, or stiff. There may be areas of thickened skin (corns or calluses) on top of or between the toes, a callus may also be observed at the tip of the affected toe beneath the toenail. An attempt to passively correct the deformity will help elucidate the best treatment option as the examiner determines whether the toe is still flexible or not. It is advisable to assess palpable pulses, since their presence is associated with a good prognosis for healing after surgery. X-rays will demonstrate the contractures of the involved joints, as well as possible arthritic changes and bone enlargements (exostoses, spurs). X-rays of the involved foot are usually performed in a weight-bearing position.
Non Surgical Treatment
Putting padding between your toes and strapping them in place can help to stop pain caused by the toes rubbing. Custom-made insoles for your shoes will help to take the pressure off any painful areas. Special shoes that are wider and deeper than normal can stop your toes rubbing. However if your pain persists your consultant may recommend an surgery.
Surgical Treatment
There are several surgical techniques used to treat hammertoes. When the problem is less severe, the doctor will remove a small piece of bone at the involved joint and realign the toe joint. More severe hammer toes may need more complicated surgery.
Bunions Treatment Surgery
Overview
 Hallux valgus may sound like a curse from Harry Potter, but it?s the medical term for a bunion, a bony growth where the big toe joins the foot. At best a bunion is an unsightly bump which can get a bit red and sore. If it gets big enough it limits the type of shoes you can wear, and sometimes a painful sac of fluid known as a bursa develops around it. But left untreated, a bunion really can become a curse if it starts to push the big toe towards the smaller ones, causing more problems such as hammer toes, or problems in the spine and legs.
Hallux valgus may sound like a curse from Harry Potter, but it?s the medical term for a bunion, a bony growth where the big toe joins the foot. At best a bunion is an unsightly bump which can get a bit red and sore. If it gets big enough it limits the type of shoes you can wear, and sometimes a painful sac of fluid known as a bursa develops around it. But left untreated, a bunion really can become a curse if it starts to push the big toe towards the smaller ones, causing more problems such as hammer toes, or problems in the spine and legs.
Causes
The most common cause of bunions is wearing shoes that are too tight. The condition is not hereditary, but it does tend to run in families-often due to a faulty foot structure. Other causes of this condition might be neuromuscular problems, flat feet, pronated feet, or foot injuries.
Symptoms
A bulging bump on the outside of the base of your big toe. Swelling, redness or soreness around your big toe joint aggravated by footwear. Red, calloused skin along the inside edge of the big toe. Corns or calluses under the ball of the foot or where the first and second toes overlap. Persistent or intermittent pain. Restricted movement of your big toe.
Diagnosis
People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen.
Non Surgical Treatment
There are a number of treatment options for bunions. Non-surgical treatments are usually tried first, including painkillers, orthotics (insoles) and bunion pads. However, these can only help to reduce the symptoms of bunions, such as pain. They don't improve the appearance of your foot. 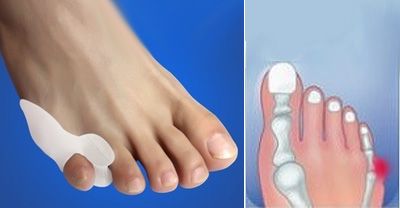
Surgical Treatment
Bunion surgery can be performed under local or general anaesthetic. The operation usually takes between half an hour to an hour. There are several types of bunionectomies. Some involve removal and realignment of the bones in your foot. Mild bunion problems can sometimes be resolved using soft tissue release or tightening. For some very severe cases bones of the big toe are fused or the bunion is cut out along with some of the bone at the base of the toe. Be sure and discuss which type of operation you will have with your surgeon. With any type of bunionectomy your surgeon will make one or more incisions (cuts) near your big toe. They will use instruments to trim the bones and remove the bunion. Wire, screws or plates may also be used to hold the new joint in place.
Prevention
Here are some tips to help you prevent bunions. Wear shoes that fit well. Use custom orthotic devices. Avoid shoes with small toe boxes and high heels. Exercise daily to keep the muscles of your feet and legs strong and healthy. Follow your doctor?s treatment and recovery instructions thoroughly. Unfortunately, if you suffer from bunions due to genetics, there may be nothing you can do to prevent them from occurring. Talk with your doctor about additional prevention steps you can take, especially if you are prone to them.
Do I Suffer From Overpronation Of The Foot
Overview
Your feet are the foundation for your entire body. When this foundation is misaligned or functioning poorly the effects can be felt throughout the body, whether in muscle and joint pain or through more serious injuries. Over 75% of the population suffers from overpronation or excessive supination, yet most of us are unaware of our own foot type and how it affects the rest of our body.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Not all foot injuries affecting runners are necessarily down to a particular running gait; it is rarely that simple to diagnose how a foot problem developed . Simply being an overpronator does not mean that a foot injury has been caused by the running gait and it could be due to a number of factors. However mild to severe overpronators tend to be at a higher risk of developing musculoskeletal problems due to the increased stresses and strains which are placed on the body when the foot does not move in an optimum manner. The following injuries are frequently due to overpronation of the feet. Tarsal tunnel syndrome. Shin splints. Anterior compartment syndrome. Plantar fasciitis. Achilles tendonitis. Bunions. Sesamoiditis. Stress fractures. Back and hip pain. Ankle pain.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Not all over pronation is treated. Although, when it appears to be a causitive factor that is contributing to pain,or development of structural deformities, there are various degrees of treatment.In some cases specific shoes may be all that is required. In other cases, paddings or strapping, are prescribed and where necessary orthotic therapy. A podiatric assesment would be advised to asses this.
Prevention
Strengthen the glutes to slow down the force of the foot moving too far inward. Most individuals who over-pronate have weak glute muscles and strengthening this area is a must. A simple exercise to strengthen glutes is lateral tube walking across a field/court/room. Place a lateral stretch band around your ankles and move your leg sideways while keeping your feet forward.
Your feet are the foundation for your entire body. When this foundation is misaligned or functioning poorly the effects can be felt throughout the body, whether in muscle and joint pain or through more serious injuries. Over 75% of the population suffers from overpronation or excessive supination, yet most of us are unaware of our own foot type and how it affects the rest of our body.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Not all foot injuries affecting runners are necessarily down to a particular running gait; it is rarely that simple to diagnose how a foot problem developed . Simply being an overpronator does not mean that a foot injury has been caused by the running gait and it could be due to a number of factors. However mild to severe overpronators tend to be at a higher risk of developing musculoskeletal problems due to the increased stresses and strains which are placed on the body when the foot does not move in an optimum manner. The following injuries are frequently due to overpronation of the feet. Tarsal tunnel syndrome. Shin splints. Anterior compartment syndrome. Plantar fasciitis. Achilles tendonitis. Bunions. Sesamoiditis. Stress fractures. Back and hip pain. Ankle pain.
Diagnosis
Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.
Non Surgical Treatment
Not all over pronation is treated. Although, when it appears to be a causitive factor that is contributing to pain,or development of structural deformities, there are various degrees of treatment.In some cases specific shoes may be all that is required. In other cases, paddings or strapping, are prescribed and where necessary orthotic therapy. A podiatric assesment would be advised to asses this.
Prevention
Strengthen the glutes to slow down the force of the foot moving too far inward. Most individuals who over-pronate have weak glute muscles and strengthening this area is a must. A simple exercise to strengthen glutes is lateral tube walking across a field/court/room. Place a lateral stretch band around your ankles and move your leg sideways while keeping your feet forward.
Severs Disease The Facts
Overview
Severs disease or calcaneal apophysitis causes heel pain usually in growing children between age nine and fourteen. It occurs as a result of disturbance during the final development of the heel growth plate. During this time the achilles tendon is pulling strongly on the heel bone and this excessive force can cause inflammation and pain.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease, External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, worsening of pain after exercise, a tender swelling or bulge on the heel that is sore to touch, calf muscle stiffness first thing in the morning, limping, a tendency to tiptoe.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The primary method of treating Sever?s disease is taking time off from sports and other physical activities to alleviate the pressure on the heel bone. During the healing period, your child?s doctor may also recommend physical therapy or any type of exercise that involves stretching and strengthen leg muscles and tendons. Wrapping ice in a towel and placing it under the child?s heel will also help to alleviate and reduce pain and swelling.
Severs disease or calcaneal apophysitis causes heel pain usually in growing children between age nine and fourteen. It occurs as a result of disturbance during the final development of the heel growth plate. During this time the achilles tendon is pulling strongly on the heel bone and this excessive force can cause inflammation and pain.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease, External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, worsening of pain after exercise, a tender swelling or bulge on the heel that is sore to touch, calf muscle stiffness first thing in the morning, limping, a tendency to tiptoe.
Diagnosis
Low-grade inflammation of the calcaneal apophysis cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in children with Sever's disease these x-rays are usually normal. Advanced Sever's disease can be seen on x-ray but usually the problem is treated before it reaches this point. Other diagnostic tests, such as bone scans or MRI's, are not usually required in typical cases of Sever's disease. These, or other tests, may be required to rule out other conditions, such as stress fractures of the calcaneus or other bony abnormalities that can mimic Severs disease.
Non Surgical Treatment
The primary method of treating Sever?s disease is taking time off from sports and other physical activities to alleviate the pressure on the heel bone. During the healing period, your child?s doctor may also recommend physical therapy or any type of exercise that involves stretching and strengthen leg muscles and tendons. Wrapping ice in a towel and placing it under the child?s heel will also help to alleviate and reduce pain and swelling.
Achilles Tendon Rupture Rehabilitation Schedule
Overview
 The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.
The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.
Causes
There are a number of factors that can increase the risk of an Achilles tendon rupture, which include the following. You?re most likely to rupture your Achilles tendon during sports that involve bursts of jumping, pivoting and running, such as football or tennis. Your Achilles tendon becomes less flexible and less able to absorb repeated stresses, for example of running, as you get older. Small tears can develop in the fibres of the tendon and it may eventually completely tear. There is a very small risk of an Achilles tendon rupture if you have Achilles tendinopathy (also called Achilles tendinitis). This is where your tendon breaks down, which causes pain and stiffness in your Achilles tendon, both when you exercise and afterwards. If you take quinolone antibiotics and corticosteroid medicines, it can increase your risk of an Achilles tendon injury, particularly if you take them together. The exact reasons for this aren't fully understood at present.
Symptoms
Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel. An inability to bend your foot downward or "push off" the injured leg when you walk. An inability to stand up on your toes on the injured leg. A popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward.
Diagnosis
A staggering 20%-30% of Achilles tendon ruptures are missed. Thompson (calf squeeze) test is 96% sensitive and 93% sensitive. Unfortunately, some health practitioners fail to perform this simple clinical test. Ultrasound examination or an MRI can confirm an Achilles tendon rupture.
Non Surgical Treatment
Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months. 
Surgical Treatment
Surgery could allow for a quicker healing time. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the tissue, the repair may be reinforced with other tendons. As with any surgery, the main complication is the risk for infection, however, this risk is reduced by using smaller incisions.
Prevention
The following can significantly reduce the risk of Achilles tendon rupture. Adequate stretching and warming up prior to exercising. If playing a seasonal sport, undertake preparatory exercises to build strength and endurance before the sporting season commences. Maintain a healthy body weight. This will reduce the load on the tendon and muscles. Use footwear appropriate for the sport or exercise being undertaken. Exercise within fitness limits and follow a sensible exercise programme. Increase exercise gradually and avoid unfamiliar strenuous exercise. Gradual ?warm down? after exercising.
Fixing Flat Feet In Adults
Overview
A more serious condition, according to ACFAS, is adult-acquired flatfoot, often cause by posterior tibial tendon dysfunction (PTTD). In this case, the tendon that supports the arch weakens and fails, leading to a rigid flatfoot where the arch stays flat even when you aren't standing. It can lead to a loss of range of motion in the foot and ankle and pain in the arch. The ACFAS clinical guideline recommends that flatfoot caused by PTTD can be treated with custom shoe orthotics, soft casts, walking boots, physical therapy and non-steroidal anti-inflammatory medications. If there is no relief or the condition worsens, then the patient may be referred to surgery. 
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot.
Diagnosis
Although you can do the "wet test" at home, a thorough examination by a doctor will be needed to identify why the flatfoot developed. Possible causes include a congenital abnormality, a bone fracture or dislocation, a torn or stretched tendon, arthritis or neurologic weakness. For example, an inability to rise up on your toes while standing on the affected foot may indicate damage to the posterior tibial tendon (PTT), which supports the heel and forms the arch. If "too many toes" show on the outside of your foot when the doctor views you from the rear, your shinbone (tibia) may be sliding off the anklebone (talus), another indicator of damage to the PTT. Be sure to wear your regular shoes to the examination. An irregular wear pattern on the bottom of the shoe is another indicator of acquired adult flatfoot. Your physician may request X-rays to see how the bones of your feet are aligned. Muscle and tendon strength are tested by asking you to move the foot while the doctor holds it.
Non surgical Treatment
Because of the progressive nature of PTTD, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery and progression of your condition can be arrested. In contrast, untreated PTTD could leave you with an extremely flat foot, painful arthritis in the foot and ankle, and increasing limitations on walking, running, or other activities. In many cases of PTTD, treatment can begin with non-surgical approaches that may include orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. 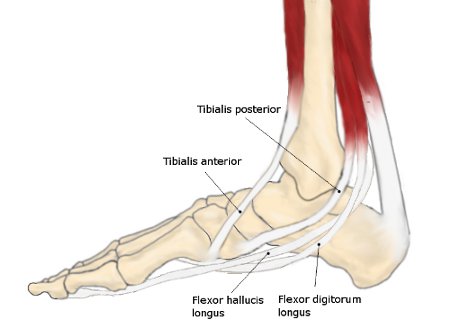
Surgical Treatment
Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle.